Dysmenorrhea cramps are common when it’s that time of the month. However, if severe pain occurs, it might be one of the endometriosis symptoms. Endometriosis pain is one of the symptoms of endometriosis that you should monitor, especially if the pain severity is unbearable.
In the Philippines, where period pain is still widely treated as something you’re supposed to just power through, that gap is even wider. Discover when it’s time to consult a doctor by acknowledging the threat of endometriosis pain to your reproductive health. Let’s begin!
What is Endometriosis?
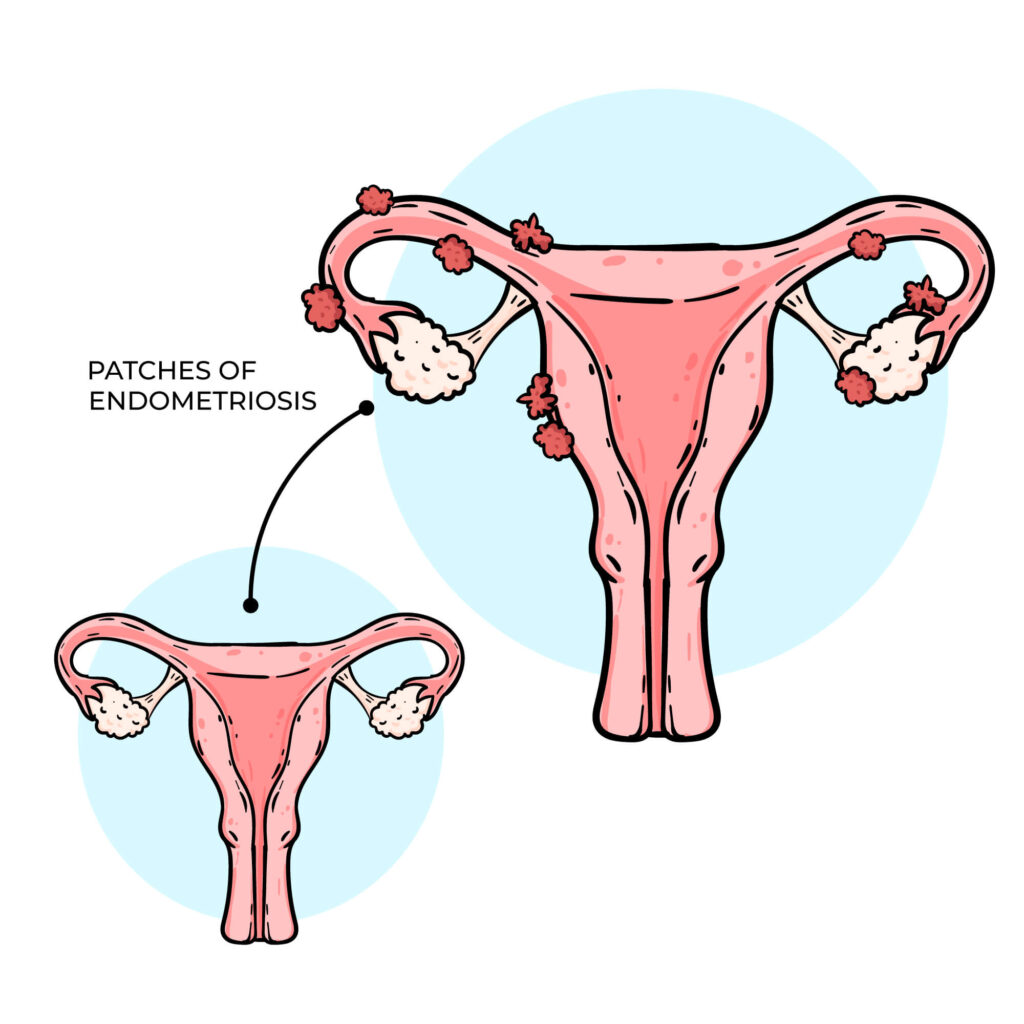
Endometriosis is a chronic condition where tissue similar to the endometrium (the lining of your uterus) grows outside the uterus. These growths, called endometriosis lesions, most commonly appear on the ovaries, fallopian tubes, the outer wall of the uterus, and the tissue lining your pelvic cavity. In some cases, they spread to the bowel, bladder, or even the diaphragm.
The pain comes from what these lesions do every menstrual cycle. They respond to your hormones the same way your uterine lining does: they thicken, break down, and bleed. But unlike your period, that blood has no way to leave your body. It pools inside the pelvic cavity, irritating surrounding tissue and triggering an inflammatory response that builds over time.
Where Do You Feel Endometriosis Pain?
Pelvic pain from endometriosis is most commonly felt in the lower abdomen, around the ovaries, and across the lower back. It can also show up during bowel movements, urination, or deep intercourse, depending on where the lesions have grown. In rarer cases where tissue reaches the diaphragm, the pain can radiate to the upper abdomen or shoulder.
The sensation ranges from a dull, throbbing ache to sudden sharp stabs. When lesions press on or grow into nerves, some women report burning or tingling that shoots down the legs or hips.
Visit a specialist if you have endometriosis as it is also one of the reasons for infertility in women. Read this related article to better take care of your reproductive health.

How Endometriosis Pelvic Pain Differs From Regular Period Cramps?
Most women experience some degree of menstrual cramps. The uterus contracts to shed its lining, and that causes discomfort. For most, it’s manageable with a heating pad or a standard dose of ibuprofen. However, the pain caused by endometriosis is very different.
- It tends to be more severe and less responsive to over-the-counter painkillers
- It often starts days before your period begins and continues after bleeding stops
- It gets progressively worse over months and years instead of staying consistent
- It frequently shows up outside of your period, including during ovulation, after sex, or during bowel movements
- It can affect areas beyond the uterus, including the lower back, legs, and abdomen
The word doctors use for severe menstrual pain is dysmenorrhea. When that pain is caused by endometriosis rather than normal uterine contractions, it’s classified as secondary dysmenorrhea, meaning there’s an underlying condition driving it.
Why Chronic Pelvic Pain Endometriosis Occurs: What Causes Endometriosis Pain
Endometriosis pain isn’t caused by one single mechanism. Several biological processes work together to create the pain experience, and understanding them helps explain why the condition is so variable from person to person.
Inflammation and the immune response
Every time endometriosis lesions bleed during your menstrual cycle, the trapped blood irritates surrounding tissue. Your immune system responds by sending inflammatory chemicals to the area. Over time, this creates a chronic inflammatory environment in your pelvis.
This inflammation doesn’t just cause pain at the lesion sites. It makes nearby nerve endings hypersensitive, meaning they fire pain signals more easily and more often. That’s why endometriosis patients sometimes feel pain from activities that shouldn’t hurt, like walking, sitting for extended periods, or simply wearing tight clothing around the waist.
Scar tissue and adhesions
Repeated cycles of bleeding, inflammation, and healing produce scar tissue called adhesions. These adhesions can glue organs together. For instance, your ovary might become stuck to your pelvic wall or your fallopian tubes might become kinked or blocked.
When organs that are supposed to move independently get bound together, every movement pulls on those adhesions. That pulling creates a pain that worsens with certain movements or postures. This scar tissue pain can persist even when the endometriosis lesions themselves aren’t actively bleeding.
Nerve involvement
Endometriosis lesions can grow directly into or next to nerves. When this happens, the result is neuropathic pain, a type of pain caused by nerve damage rather than tissue injury. Neuropathic pain often feels different from inflammatory pain. Women describe it as burning, shooting, electric, or tingling.
Nerve involvement also explains why endometriosis pain can radiate to unexpected places. The pelvic nerves share pathways with nerves that serve the legs, lower back, and even the diaphragm. When a lesion irritates a pelvic nerve, your brain can interpret that signal as pain in your hip, thigh, or shoulder.
Hormone fluctuations
Endometriosis is an estrogen-dependent condition. Higher estrogen levels fuel the growth of endometriosis lesions, while the hormonal shifts of your menstrual cycle trigger the bleeding-inflammation-pain cycle.
This hormonal connection explains why endometriosis pain typically follows a cyclical pattern, peaking around menstruation when hormone levels shift dramatically. It also explains why hormonal treatments that lower estrogen levels or suppress ovulation can provide significant pain relief.
Consult an endocrinologist to help regulate your hormones.
Pelvic floor dysfunction
Living with chronic pelvic pain often causes a secondary problem: the pelvic floor muscles tighten up as a protective response. Over months and years, this guarding reflex can lead to pelvic floor dysfunction, where the muscles become chronically tense, weak, or uncoordinated.
Pelvic floor dysfunction adds its own layer of pain on top of the endometriosis. It can cause pain during sex, difficulty with bowel movements, urinary urgency, and a constant feeling of pressure or heaviness in the pelvis. This is one reason why treating endometriosis sometimes requires addressing the pelvic floor separately.
Is This Pain Serious? Signs that Warrant a Doctor Visit
Period pain exists on a spectrum. Mild cramping that resolves with rest or a standard painkiller is generally not a cause for concern. But endometriosis pain crosses into territory that deserves medical evaluation.
Here are the specific signs that should prompt you to schedule an appointment with an OB-GYN.
Your pain has been getting progressively worse
This is one of the most telling signs. Normal menstrual cramps tend to stay relatively stable from year to year. Endometriosis pain follows an upward curve. If your cramps at 30 are noticeably worse than they were at 22, and the trend has been consistently worsening, that progression points toward something beyond normal dysmenorrhea.
Painkillers have stopped helping
When ibuprofen, mefenamic acid, or naproxen no longer take the edge off your menstrual pain, your body is telling you the pain source goes deeper than routine uterine contractions. Endometriosis pain can become resistant to standard pain relief because it involves inflammation, adhesions, and nerve irritation that NSAIDs weren’t designed to address fully.
You have pain outside your period
Chronic pelvic pain that shows up mid-cycle, during ovulation, or on random days with no connection to your menstrual cycle suggests the condition has progressed. Chronic pelvic pain endometriosis is a sign that inflammation and adhesions have built up enough to cause ongoing discomfort regardless of where you are in your hormonal cycle.
Sex is painful
Deep pain during or after intercourse isn’t something you need to accept. Dyspareunia associated with endometriosis typically involves pain that’s felt deep inside rather than at the entrance, and it often lingers for hours afterward. This symptom points to lesions in specific locations (behind the uterus or along the uterosacral ligaments) and it rarely improves without treatment.
Bowel or bladder symptoms follow your cycle
If you notice bloating, constipation, diarrhea, pain during bowel movements, or urinary symptoms that consistently worsen around your period, endometriosis affecting the bowel or bladder could be the cause. Many women get misdiagnosed with irritable bowel syndrome (IBS) before anyone considers endometriosis.
Read this related article to know more about IBS
You’ve been trying to get pregnant without success
Endometriosis is found in 30% to 50% of women experiencing infertility. The condition can block fallopian tubes with adhesions, damage egg quality through chronic inflammation, and create a hostile environment for implantation. If you’ve been trying to conceive for 12 months (or 6 months if you’re over 35) without success and you have painful periods, ask your doctor about an endometriosis evaluation.
Your pain affects your ability to function
If endometriosis pain is causing you to miss work or school, cancel commitments, avoid physical activity, or withdraw from relationships, that functional impact is reason enough to seek help. Pain that controls your schedule is not normal period pain. It’s a medical symptom that deserves investigation.
Medical Treatment Options for Endometriosis Pain
There’s no cure for endometriosis yet. But there are effective ways to manage the pain and slow the disease. Your doctor will recommend a treatment plan based on your symptom severity, the extent of the disease, your age, and whether pregnancy is a goal.
Over-the-counter and Prescription Pain Relief
For mild to moderate endometriosis pain, nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen are the typical starting point. These reduce both pain and inflammation, and they work best when taken preemptively, starting a day or two before your period rather than waiting for the pain to peak.
When NSAIDs fall short, your doctor may prescribe stronger options or refer you to a pain specialist who can develop a more targeted approach. The goal isn’t just masking pain. It’s breaking the cycle of inflammation that makes each month worse than the last.
Hormone Therapy
Because endometriosis feeds on estrogen, many treatments aim to lower estrogen levels or stop ovulation entirely, slowing lesion growth and reducing the monthly bleeding-inflammation cycle.
Common hormonal approaches include:
- Combined oral contraceptives taken continuously (skipping the placebo week) to reduce or eliminate periods
- Progestin-only methods (pills, hormonal IUD, injection, or implant) to thin the endometrial tissue and lower inflammation
- GnRH agonists and antagonists to create a temporary menopause-like state by suppressing estrogen production. These are usually short-term due to side effects like bone density loss and hot flashes
Hormonal therapy works well for pain management in many women, but it’s not a permanent fix. Symptoms often return after stopping treatment, and these options aren’t suitable if you’re actively trying to conceive.
Surgical treatment
Laparoscopic surgery is both a diagnostic and treatment tool for endometriosis. During the procedure, a surgeon makes small incisions in the abdomen, inserts a camera, and directly visualizes the endometriosis lesions. The surgeon can then remove or destroy the lesions and cut away adhesions binding organs together.
For many women with moderate to severe endometriosis, surgery combined with hormonal therapy afterward produces the longest stretch of symptom relief. Some women experience years of reduced pain following a successful excision surgery. However, when severe scenario comes, and pregnancy is no longer a goal, hysterectomy (removal of the uterus) may be discussed.
Physical Therapy for the pelvic floor
Many endometriosis patients develop pelvic floor dysfunction as a secondary effect of chronic pain. The muscles tighten, weaken, or lose coordination over time. Physical therapy with a pelvic floor specialist can address this. Treatment typically involves manual therapy to release tight muscles, targeted exercises, biofeedback training, and relaxation techniques.
Take note that pelvic floor physical therapy doesn’t treat endometriosis directly, but it can significantly reduce the muscle-related pain layered on top of it. Many women find that combining pelvic floor work with medical treatment gives better results than either one alone.
Lifestyle Adjustments that Support Treatment
Aside from procedures and medical treatments of endometriosis, you can also manage endometriosis pain and other symptoms of endometriosis through lifestyle changes. This includes starting a more active and healthy life.
- Regular exercise: It increases blood flow to the pelvic area, releases endorphins, and can help regulate estrogen levels. You don’t need intense workouts. Walking, swimming, yoga, and gentle stretching at a consistent pace (150 minutes per week) are enough. Many women also report that exercise helps with the fatigue and low mood that accompany endometriosis.
- Healthy diet: On the nutrition side, endometriosis is an inflammatory condition, so reducing dietary inflammation can help. Research supports diets rich in omega-3 fatty acids (fish, walnuts, flaxseed), colorful fruits and vegetables, and whole grains. Some women notice improvement when they cut back on red meat, processed foods, alcohol, and caffeine. There’s no single proven “endometriosis diet,” but the principle of less inflammatory food, less inflammatory pain holds up.
- Heat therapy: Applying warmth to the lower abdomen or back relaxes uterine smooth muscle and increases local blood flow, reducing cramping. Heating pads, warm baths, and adhesive heat patches all work.
- Stress management: Chronic stress also amplifies pain perception and fuels inflammation. Building a stress management practice, whether that’s deep breathing, meditation, adequate sleep, or time doing something you enjoy, can lower your pain baseline over time.
Consult a specialist today to know more of the appropriate endometriosis treatment available in the Philippines. Book your appointment on NowServing to address your endometriosis pain immediately.
Read this article if you want to have a more balanced diet with Go, Grow, and Glow Foods.
How to Book a Consultation on NowServing
If you’ve recognized yourself in any of the symptoms described above, the next step is getting evaluated by a specialist. Here’s how to do that through NowServing.
Finding the right specialist
For suspected endometriosis, an OB-GYN is your first stop. They can perform an initial evaluation, order imaging, start hormonal treatment, and refer you for surgery if needed.
If your situation involves infertility, complex disease, or symptoms that haven’t responded to initial treatment, a reproductive endocrinology and infertility specialist may be the better fit. These doctors have advanced training in hormonal conditions and reproductive surgery.
Booking through the platform
NowServing lets you search for doctors by specialty, location, hospital affiliation, and HMO coverage. This allows you to easily find the specialist you need. You can also book an online consultation if you prefer that than in-person doctor visit.
Read this related article to know how you can book an online consultation with an OBGYN.
Here’s how to book an endometriosis doctor on NowServing
- Access the endometriosis page on NowServing or open the NowServing app
- Browse the list of specialists in the Philippines that can manage endometriosis
- Fill-up the form provided
- Wait for the doctor to accept your booking.
If you feel your concerns are being dismissed, get a second opinion. Endometriosis is underdiagnosed precisely because pain is so often brushed off as “just cramps.”
Find and book other specialists on NowServing with this guide.
Frequently Asked Questions
What is endometriosis belly? Why does it happen?
Endometriosis belly is a term women in online communities use to describe the severe bloating that comes with the condition. Your abdomen can swell to the point where you look several months pregnant, often within hours. This bloating is driven by the inflammatory response in your pelvis and can be accompanied by gas, nausea, and general abdominal discomfort.
The bloating tends to worsen around your period but can occur at any time. It’s different from typical period bloating in both its severity and how quickly it appears and disappears.
Can endometriosis pain be managed without surgery?
Yes. Many women manage endometriosis pain effectively with a combination of NSAIDs, hormonal therapy (birth control pills, hormonal IUD, or GnRH therapy), pelvic floor physical therapy, and lifestyle adjustments like regular exercise and anti-inflammatory eating. Surgery is typically recommended when these approaches don’t provide adequate relief or when endometriosis is affecting fertility.
Does endometriosis always get worse over time?
Not always. Some women have stable disease that doesn’t progress significantly. Others experience gradual worsening, especially if estrogen levels remain high and no treatment is started. Hormonal therapy can slow or stop progression in many cases. After menopause, when estrogen levels drop naturally, symptoms often improve, though this isn’t guaranteed for every woman.
Can I still get pregnant if I have endometriosis?
Many women with endometriosis do conceive, either naturally or with fertility assistance. The impact depends on severity and location. Mild cases may not affect your chances significantly. Severe disease involving blocked fallopian tubes or damaged ovaries may require assisted reproductive technology like IVF. A fertility specialist can evaluate your specific situation and recommend the best approach.
When should I go to the emergency room for endometriosis pain?
Go to the ER if you experience sudden, severe abdominal pain that’s different from your usual endometriosis pain (this could indicate an ovarian cyst rupture or torsion), heavy vaginal bleeding that soaks through a pad every hour, fever combined with pelvic pain, or fainting and dizziness with pain. These require immediate evaluation regardless of your endometriosis history.
Can endometriosis kill you?
Endometriosis is not a fatal condition. It can, however, lead to complications that need urgent attention: ovarian cysts (endometriomas) can rupture, severe adhesions may obstruct the bowel, and research has found a small link to certain ovarian cancers, though the overall risk stays low.
For most women, the bigger concern is how endometriosis erodes daily life, fertility, and mental health over time. Seeing a specialist early gives you the best chance of managing symptoms before they escalate.
Conclusion
Endometriosis pain is real and you should know its difference from menstruation cramps. Your pain deserves answers. And with over 10 million patients in its network, NowServing can help you find the specialist to provide them.
Book a doctor consultation with an OBGYN today to get diagnosed with endometriosis.